Meeting date: October 3, 2018
Prepared by: Michael Whyte, Health Promotion Specialist, Health Analytics; Jennifer Macleod, Manager, Health Analytics
Report no.: BH.01.OCT0318.R30
Approved by: Dr. Kyle Wilson, Director, Information Systems & Chief Privacy Officer
Submitted by: Dr. Nicola J. Mercer, MD, MBA, MPH, FRCPC, Medical Officer of Health and CEO
Recommendations
It is recommended that the Board of Health:
- Receive this report for information.
Key Points
In 2017, the number of opioid-related Emergency Department (ED) visits and mortality have reached its highest point in Wellington County, Dufferin County and the City of Guelph (WDG).
- The Ontario Prescription Opioid tool is a new, publicly available resource.1 This tool presents different indicators that describe opioid-prescribing trends across Ontario. In WDG, the amount of dispensed opioids for pain has decreased from 2013 to 2017.
- Wellington-Dufferin-Guelph Public Health (WDGPH) has coordinated with 9 organizations to create an Early Warning Opioid-Surveillance System for the City of Guelph. WDGPH anticipates this will help to identify and share information about new patterns of overdoses including possible local tainted drug supplies or counterfeit pharmaceuticals.
-
WDGPH is continuing to search for opportunities to create partnerships with community partners in Dufferin County and Wellington County to support opioid surveillance.
Discussion
Background
This report is meant as an update for the Board of Health on matters of opioid-related events within WDG with regards to:
- Surveillance
- Community Partnerships to Improve Surveillance Timeliness
Surveillance
In order to understand the needs of the community, WDGPH is continually monitoring trends in relation to current opioid-related harms in WDG and across the province. WDGPH has identified several sources of information that help identify the impact that opioids and their related harms have in WDG. This information allows WDGPH to better support those who are most impacted by opioid related harms by supporting strategic collaboration with key community partners in the development of initiatives designed to deliver services to priority populations.
This section outlines WDGPH’s current understanding of opioid-related harms through the available data.
Opioid-Related Emergency Department Visits
Across the province overdose and death related to opioid use has been increasing steadily. In 2017, the rate of opioid-related emergency department (ED) visits, in Ontario, was 54.5 per 100,000 people, approximately triple the rate for the province in 2007 (17.5 per 100,000 – Figure 1). In WDG, there is a similar increase as the rate for ED visits rose from 16.9 per 100,000 residents in 2007, to 52.5 per 100,000 residents in 2017. The largest increase in rates are between 2016 and 2017, where ED visits for opioid-related events increased more than 50% in both the province of Ontario and within WDG.
Figure 1: Rate per 100,000 Residents of Opioid-Related Emergency Department Visits in Wellington-Dufferin-Guelph Compared to Ontario, By Year, 2003-2017
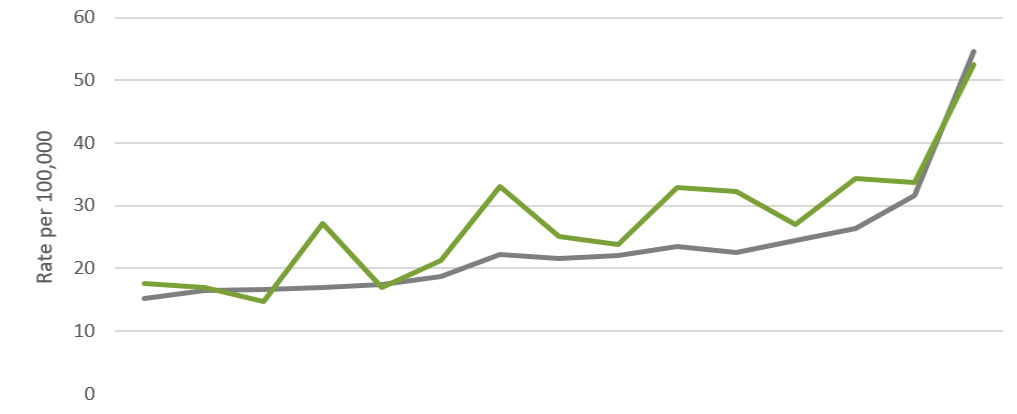
Grey - Ontario, Green - WDG
Data source: National Amulatory Care Reporting System (NACRS). 2003-2017, Ontario Ministry of Health and Long Term Care, IntelliHEALTH Ontario; accessed August 23, 2018.
| 2003 | 2004 | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Ontario | 15.2 | 16.5 | 16.7 | 17 | 17.5 | 18.7 | 22.2 | 21.6 | 22.1 | 23.5 | 22.5 | 24.5 | 26.3 | 31.7 | 54.6 |
| WDG | 17.6 | 17 | 14.8 | 27.2 | 16.9 | 21.3 | 33.1 | 25.1 | 23.8 | 32.9 | 32.3 | 27 | 34.3 | 33.7 | 52.5 |
Data source: National Ambulatory Care Reporting System (NACRS). 2003-2017, Ontario Ministry of Health and Long Term Care, IntelliHEALTH Ontario; accessed August 23, 2018.
Opioid-related ED visits have increased in Ontario and in WDG (Figure 2). The greatest difference seen between 2016 and 2017 is in the City of Guelph, where the rate had doubled from 2016 to a rate of 74.6 per 100,000 residents in 2017. The rate of opioid-related ED visits in the City of Guelph is 37% higher than the average for Ontario, 82% higher than that of Dufferin County and 155% higher than that of Wellington County in 2017.
Figure 2 - Rate per 100,000 Residens of Opioid-Related Emergency Department Visits in Wellington County*, Dufferin County and the City of Guelph Compared to Ontario, By Year, 2003-2017.
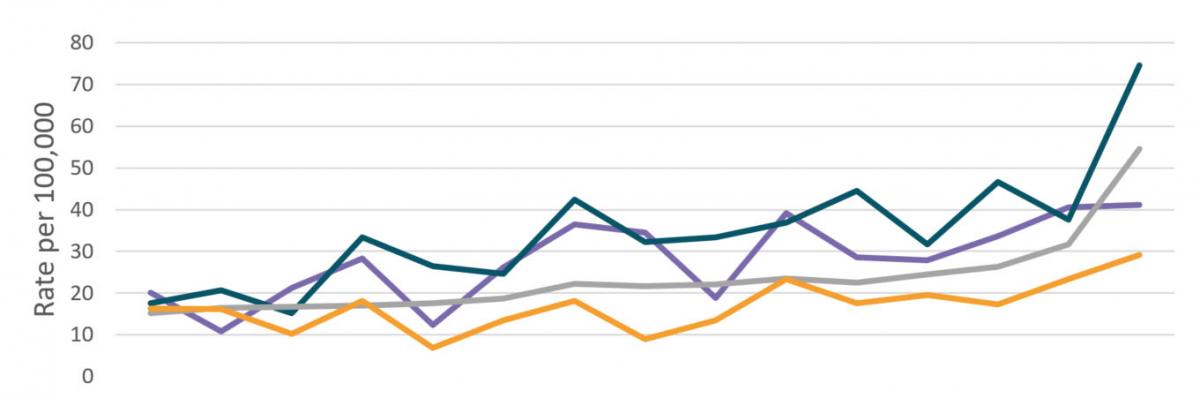
Purple - Dufferin, Teal - Guelph, Grey - Ontario, Orange - Wellington
| 2003 | 2004 | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Dufferin | 20.1 | 10.8 | 21.3 | 28.3 | 12.3 | 26.2 | 36.5 | 34.5 | 18.8 | 39.1 | 28.6 | 27.9 | 33.6 | 40.6 | 41.1 |
| Guelph | 17.5 | 20.6 | 15.2 | 33.4 | 26.5 | 24.6 | 42.4 | 32.2 | 33.4 | 36.9 | 44.5 | 31.7 | 46.7 | 37.6 | 74.6 |
| Ontario | 15.2 | 16.5 | 16.7 | 17 | 17.5 | 18.7 | 22.2 | 21.6 | 22.1 | 23.5 | 22.5 | 24.5 | 26.3 | 31.7 | 54.6 |
| Wellington | 16.3 | 16.1 | 10.2 | 18.1 | 6.8 | 13.5 | 18.1 | 9 | 13.5 | 23.3 | 17.6 | 19.6 | 17.3 | 23.4 | 29.2 |
*Wellington County does not include the City of Guelph
Data source: National Ambulatory Care Reporting System (NACRS). 2003-2017, Ontario Ministry of Health and Long Term Care, IntelliHEALTH Ontario; accessed August 23, 2018.
Shelburne and Guelph have higher than average rates of ED visits for opioid-related harms when compared to the province (74 vs. 55 ED visits per 100,000 residents). All other areas within WDG are comparable to the provincial average.
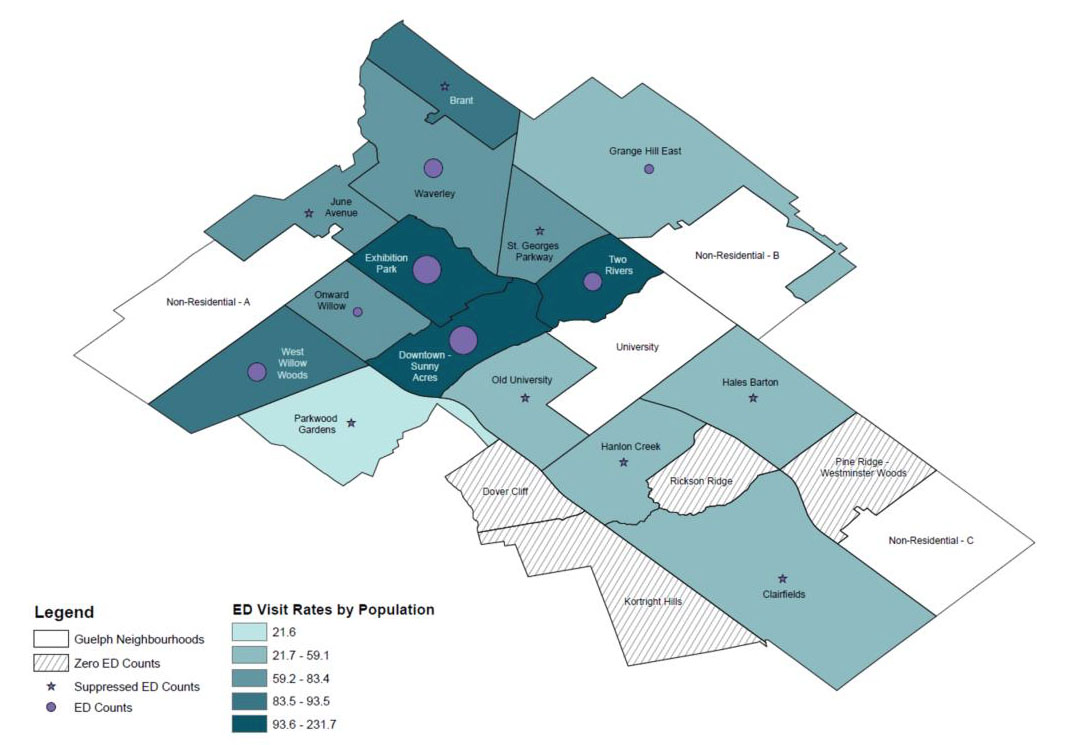
To better understand the rate of ED visits in the City of Guelph in 2017, WDGPH has mapped ED visits by neighbourhood (Figure 3). This data only includes people who have visited the ED and does not include those who do not use emergency medical services. It is also important to note that those who are homeless will not appear on the map as address information was not available. The map identifies that the majority of individuals that have used emergency hospital services as a result of opioid-related harm are concentrated in the downtown section of the City.
Figure 3 - The Number, and Rate per 100,000 Residents, of Opioid-Related Emergency Department Visits in the City of Guelph by Neighbourhood, 2017
Data source - National Amulatory Care Reporting System (NACRS). 2017, Ontario Ministry of Health and Long Term Care, IntelliHEALTH Ontario; accessed August 23, 2018.
Opioid-Related Mortality
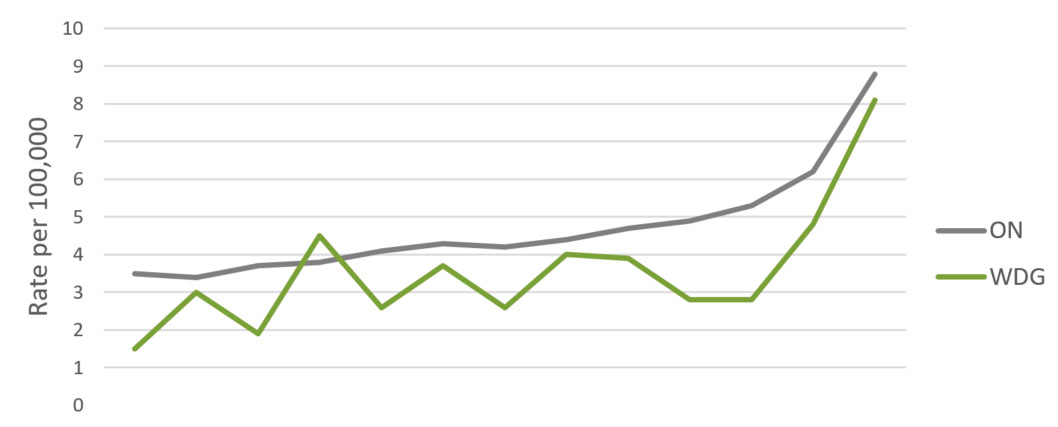
Consistent with ED visits due to opioid-related harm, mortality where an opioid was present has also increased (Figure 4). Within the past three years (2015-2017), the rate of mortality in WDG has increased from 2.8 to 8.1 per 100,000, which is approximately three times the rate that was seen in 2015.
Figure 4 (below) displays the rate of opioid-related death for the province of Ontario and WDG. Information from August 2017 to December 2017 is still considered preliminary and may change slightly as cases are confirmed. However, this data provides the best understanding of the more severe consequences of the use of opioids within WDG.
Figure 4 - Rate per 100,000 Residents of Opioid-Related Death in Wellingotn-Dufferin-Guelph Compared to Ontario, By Year, 2005-2017
| 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Ontario | 3.5 | 3.4 | 3.7 | 3.8 | 4.1 | 4.3 | 4.2 | 4.4 | 4.7 | 4.9 | 5.3 | 6.2 | 8.8 |
| WDG | 1.5 | 3 | 1.9 | 4.5 | 2.6 | 3.7 | 2.6 | 4 | 3.9 | 2.8 | 2.8 | 4.8 | 8.1 |
Data source: Ontario Opioid-Related Death Database, 2005-2017, Office of the Cheif Coroner for Ontario; accessed through the Interactive Opioid Tool 31 August 2018.
The Narcotics Monitoring System
The Ontario Prescription Opioid tool is a publicly available resource developed by the Ontario Drug Policy and Research Network (ODPRN) in collaboration with Public Health Ontario (PHO).1 The tool uses data collected in the Narcotics Monitoring System (NMS) and presents different indicators of prescription opioid dispensing from community pharmacies across Ontario.1 This section describes patterns in opioid dispenses across WDG in comparison to the province of Ontario as a whole.
Since 2013, the total amount of opioids dispensed for pain has decreased across the province of Ontario. In WDG the amount of dispensed opioid medications has decreased by 20% from 2013 to 2017, following a similar decrease of 26% for the province of Ontario.
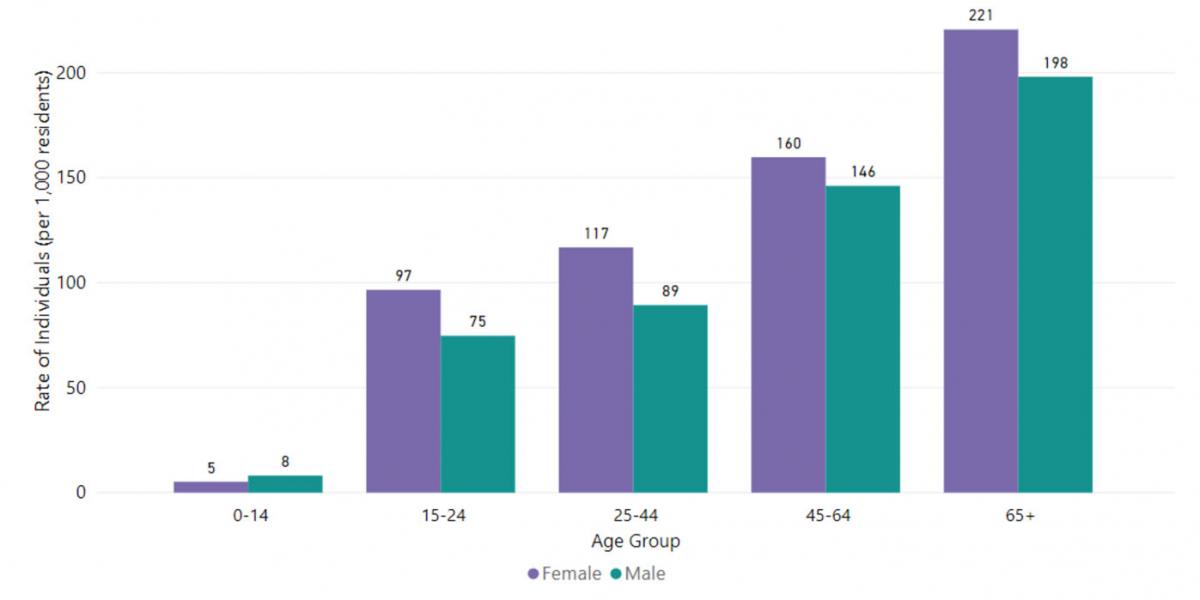
The proportion of people who are dispensed opioids increases with age. The highest proportion is within the age group of 65 and above (Figure 5). The number of women receiving opioids for pain is slightly higher than that of men in all age groups. This occurs both in WDG and the province of Ontario.
Figure 5 - Rate of Individuals per 1,000 Residents Dispensed Opioids to Treat Pain in Wellington-Dufferin-Guelph, by Age Group, 2017
Data source: Ontario Drug Policy Research Network. Ontario Prescription Opioid Tool. Toronto, ON; July 2018. DOI: 10.31027/ODPRN.2018.01. Available from: http://odprn.ca/ontario-opioid-drug-observatory/ontario-prescription-opi…
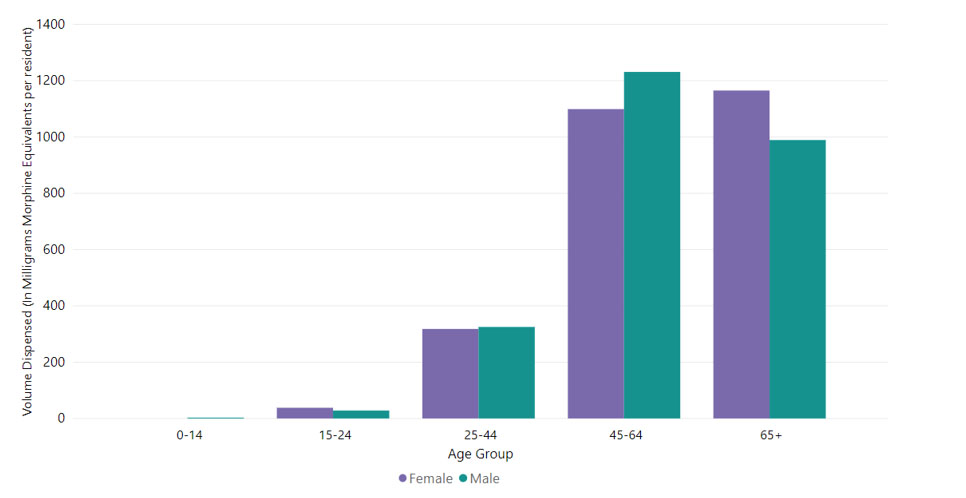
Although the proportion of people being dispensed opioids is highest within the 65+ age range, the largest amount of opioids dispensed to treat pain are being dispensed to males between the ages of 45-64 (Figure 6). Individuals aged 45 and older are receiving 85% of the total amount of opioid medication dispensed in the WDG region. Locally opioid dispensing and prescribing resemble that of the Province of Ontario as a whole.
Figure 6 - Amount of Dispensed Opioids to Treat Pain (in Milligrams Morphine Equivalents) per Resident in Wellington-Dufferin-Guelph, by Age Group, 2017
Data source: Ontario Drug Policy Research Network. Ontario Prescription Opioid Tool. Toronto, ON; July 2018. DOI: 10.31027/ODPRN.2018.01. Available from: http://odprn.ca/ontario-opioid-drug-observatory/ontario-prescription-opi…
New Community Partnerships to Improve Surveillance
On April 4, 2018, WDGPH shared with the Board of Health that WDGPH would be working closely with community partners in the development of an early warning system for opioid-related harms. This was a product of both funding provided by the Ministry of Health and Long-Term Care for enhanced early warning surveillance and a demonstrated need by community partners and organizations.
Since April, 2018, in partnership with members of the Wellington Guelph Drug Strategy (WGDS), WDGPH has developed an online survey tool to collect information about overdoses or serious negative drug use reactions. WDGPH anticipates this will help to identify and share information about new patterns of overdoses including possible local tainted drug supplies, or counterfeit pharmaceuticals.
Service providers from a small group of organizations are being asked to complete the survey when they are aware of an incident. Currently, there are 9 participating organizations who will be updating the early warning system of any drug-related events, including:
- ARCH
- Sanguen Health Centre
- Guelph Community Health Centre
- Public Health
- Hope House
- The Drop In Centre
- Wyndham House
- Specialized Outreach Services
- Family and Children’s Services
The information collected will be shared in three ways:
1) Weekly reports of overdose / negative drug reactions. These will be shared with all of the organizations listed above and any additional organizations who are members of the Wellington Guelph Drug Strategy who indicate an interest in receiving them. The first report was shared on August 15th containing information from August 1st, 2018, and will continue to be distributed weekly.
2) Alerts. These will be issued based on identification of need by WDGPH, the Guelph Community Health Centre, ARCH and the Wellington Guelph Drug Strategy. Partner agencies are encouraged to share alerts in their networks to ensure at-risk populations are reached. These established networks include communication channels such as: social media platforms, client interactions, and community boards.
3) Quarterly reports. The information will be compiled quarterly and added to the online Overdose and Drug Use Information System (ODIS).
WDGPH will be exploring opportunities to expand collaboration in Dufferin County.
Conclusion
Opioid-related harms are continuing to impact WDG and the Province of Ontario as a whole. From 2016 to 2017, every region of WDG experienced an increase in opioid-related ED visits and mortality. In an effort to gather more timely information about opioid-related harms in the community, WDGPH has partnered with nine community organizations to create an early warning system. WDGPH will continue to explore opportunities to create new community partnerships in Wellington and Dufferin counties to create early warning systems.
Ontario Public Health Standard
Population Health Assessment
“Population health assessment includes measuring, monitoring, and reporting on the status of a population’s health, including determinants of health and health inequities. Population health assessment provides the information necessary to understand the health of populations through the collaborative development and ongoing maintenance of population health profiles, identification of challenges and opportunities, and monitoring of the health impacts of public health practice.”
The board of health shall:
1. assess current health status, health behaviours, preventive health practices, health care utilization relevant to public health, and demographic indicators
2. assess trends and changes in local population health
3. use population health, determinants of health and health inequities information to assess the needs of the local population
4. tailor public health programs and services to meet local population health needs
5. provide population health information, including determinants of health and health inequities to the public, community partners, and health care providers
Surveillance
“Surveillance is the systematic and ongoing collection, collation, and analysis of health-related information that is communicated in a timely manner to all who need to know, so that action can be taken. Surveillance contributes to effective public health program planning, delivery, and management. Dissemination of surveillance analyses may take the form of reports, advisories, healthy public policy recommendations, alerts, or warnings. Surveillance has historically been associated with infectious diseases and vaccination programs, but its importance has become increasingly recognized for environmental health issues, child health, reproductive health, chronic disease prevention, and injury prevention.”
The board of health shall:
1. conduct surveillance, including the ongoing collection, collation, analysis, and periodic reporting of population health indicators
2. interpret and use surveillance data to communicate information on risks to relevant audiences
WDGPH Strategic Direction(s)
✓ Health Equity: We will provide programs and services that integrate health equity principles to reduce or eliminate health differences between population groups.
✓ Organizational Capacity: We will improve our capacity to effectively deliver public health programs and services.
✓ Service Centred Approach: We are committed to providing excellent service to anyone interacting with WDG Public Health.
✓ Building Healthy Communities: We will work with communities to support the health and well-being of everyone.
Health Equity
Health equity principles are being applied across all WDGPH opioid projects with the goal of reducing or eliminating differences in opioid-related harms between population groups. According to a study by the Public Health Agency of Canada, opioid and other drug-related overdose deaths occurred across all sociodemographic and socioeconomic groups. However, characteristics most common among those who died include.2
- a history of mental health concerns, substance use disorder, trauma, and stigma
- decreased drug tolerance
- being alone at the time of overdose
- lack of social support
- lack of comprehensive and coordinated healthcare and social service follow-up
Strategies, such as Supervised Consumption Sites, tend to engage people who are more likely to be experiencing unstable living arrangements or homelessness, mental health concerns and/or chronic substance use.3 Different approaches and strategies are needed to reach a diversity of groups who have different risk factors and different needs. WDGPH will continue to explore the needs of different population groups, and use a comprehensive and targeted approach to reduce health inequities and reduce the burden of substance related harm in the community.
References
- Ontario Prescription Opioid Tool [Internet]. Ontario Drug Policy Research Network.; 2018 [cited 2018 Sep 24]. Available from: http://odprn.ca/ontario-opioid-drug-observatory/ontario-prescription-opi…
- Special Advisory Committee on the Epidemic of Opioid Overdoses. Highlights from phase one of the national study on opioid- and other drug-related overdose deaths: insights from coroners and medical examiners [Internet]. Public Health Agency of Canada. 2018 Sept [cited: 2018 Sept 24]. Available from: https://www.canada.ca/en/public-health/services/publications/healthy-liv…
- Wellington-Dufferin-Guelph Board of Health. BOH report - BH.01.MAR0718.R06 Community Response to Opioid Harms: Considerations for Supervised Consumption Sites. [Internet]. 2018 Mar 7. [cited 2018 Sep 24]. Available from: https://www.wdgpublichealth.ca/sites/default/files/file-attachments/basi…
Appendices
None.